

Conservative approach
Lithium disilicate veneers allows a minimal intervention approach. This means that tooth preparations are limited to the enamel. The resistance will be the same as the natural tooth’s.

Find your smile
It is possible to correct aesthetic imperfections, traumas, spots and holes between your teeth due to gum disease. Everything by means of a custom-made prosthesis designed for your mouth.

High precision work
We choose a treatment plan, show you the result and then apply the veneers. The veneers are thin and will be applied by professionals specialized in smile aesthetics and dental materials.
Veneers
Ceramic dental veneers are minimally invasive adhesive restorations with high aesthetic value. Thanks to minimal preparations limited to the enamel or even without touching the tooth surface with “additional” restorations (“no-prep” technique), it is possible to fabricate veneers with an average thickness of 0.5 mm.

“No-prep” techniques permit to apply veneers without drilling the teeth but only conditioning the surfaces with dedicated adhesives. This approach is extremely conservative – in accordance with the so-called “minimal intervention dentistry” – since it does not interfere in any way with the structure and the resistance of teeth.
Obviously, specific clinical conditions are needed to carry on this technique, such as diastemas (spaces between teeth), gingival black triangles (caused by periodontitis), necessity to increase volume and/or length of the teeth.
No-prep techniques are often combined with the manufacturing of partial restorations called “additionals”: if it is not necessary to cover the entire surface of one or more teeth, it is possible to fabricate small ceramic fragments that can be luted where necessary to fill a space or restore, for example, a fractured cusp.
Likewise, today it is possible to produce very thin crowns with lithium disilicate (“full veneers”), in cases where it is necessary to cover the entire dental surface (teeth severely damaged by caries, teeth worn due to mechanical abrasion or chemical erosion, just like in case of acid food and beverages, etc.). The thickness of these crowns (up to 0.3 mm) allows for minimally invasive preparations or even for no preparation at all, without touching any dental surface with rotary burs; this approach keeps large amounts of enamel and dentin and does not require the root canal treatment of teeth to be restored with prosthetic crowns.

These restorations do not interfere with the health of periodontal tissues, since the preparations do not reach the gingival margins, and guarantee an optimal blend of the restorations, thanks to the use of highly aesthetic and metal-free materials.
Many patients visiting a dentist for aesthetic purposes are sometimes undecided about the application of dental veneers or teeth bleaching.
Practically, dental bleaching (or whitening) acts on the color and is less invasive than veneers but it does not modify the shape of teeth; conversely, dental veneers are useful in the modification of both color and shape of teeth.
Ceramic veneers allow for the correction of shape and volume abnormalities (closure of interdental black triangles and diastemas, conoid teeth), pigmentations and discoloration (such as nicotine and/or caffeine stains), discolored composite restorations (yellowish/brownish), dental malpositions and congenital defects of the enamel, (fluorosis, amelogenesis imperfecta), giving balance and fullness to the smile. Moreover, veneers allow for the restoration of proper function and occlusal guidances of teeth, lengthening fractured or worn margins due to aging. Before evaluating the use of dental veneers, it might be useful to consider alternative solutions, as selective dental bleaching (in case of deep-stained teeth) or adhesive composite restorations, whose cost is on average much less expensive than that of veneers. The latter are often used in cases of small chipping or shape variations of one or more teeth.

Contact Us
Lithium disilicate
Nowadays, modern material technologies allow for the use of various types of ceramics for the fabrication of veneers, from the traditional feldspathic ceramics, highly translucent, to the latest lithium disilicate ceramics, highly resistant. The use of clinical microscopes or magnifying systems is almost indispensable to finalize properly such restorations.


The optimal mechanical properties and the high fracture resistance of lithium disilicates allow to make veneers even in biomechanically non-ideal situations, as in patients using bite planes or in case of severe incisal wear. In these cases, only bleaching is not enough to restore the natural beauty of the smile but it is necessary to reestablish the original shape prior to the aging process.
Both feldspathic and lithium disilicate ceramics can be cemented with extremely reliable adhesive techniques, guaranteeing excellent biological integration, optimal aesthetic results and proper biomimetic, restoring the optical and mechanical characteristics of natural teeth.
DIGITAL IMPRESSION FOR DENTAL VENEERS
Since veneer preparation is a non-invasive technique that does not involve the gingival space, nowadays it is possible to use Intra Oral Scanners (IOS) to obtain digital impressions.
Unlike the traditional ones, digital impressions do not require pastes, impression materials or trays that often result bulky and uncomfortable for patients.
Intra-oral scanners are high resolution cameras that allow to detect the shape of teeth and gums as well as the color of tissues, allowing for the fabrication of veneers with a full digital workflow. This technique is very quick and comfortable and permits to check the precision of preparations in real time; moreover, in most cases this approach does not require anesthesia.

Then, the file obtained from the impression is sent to the dental laboratory that will produce the veneers with a full digital workflow. In this way, manufacturing times are reduced and it is possible to achieve highly accurate and predictable results through CAD-CAM processes (Computer Aided Design-Computer Aided Manufacturing).
 odt sig. Luigi De Stefano
odt sig. Luigi De Stefano
Aesthetic analysis
The aesthetic diagnosis is aimed at evaluating all the factors that influence a proper integration of the smile in the face of a patient. It is therefore based on a facial analysis, which allows to assess the symmetry and proportions of the face, and on a dental analysis, that allows to evaluate the relationship between the teeth and the perioral soft tissues.
The facial analysis takes into consideration the midline of the face (face-nose-chin), the bipupillary line (passing through the eye pupils) and the occlusal plane (touching the dental margins and cusps) (Fig.1). Such reference planes allow for the identification of any asymmetry which should be compensated for during the dental treatment (pendant smile line, deviations of the midline, etc).

The dental analysis includes the evaluation of several parameters concerning both the teeth and the gums:
- maxillary and mandibular midlines;
- lination of dental axes;
- intra- and inter-dental proportions;
- occlusal and incisal planes;
- level of the gingival margins;
- interdental gingival papillas;
- interdental embrasures;
- color and surface texture (of both teeth and gums).
In an ideal smile, the upper and lower midlines (Fig.2, dotted yellow line) should coincide and the longitudinal axes of the teeth (Fig.2, black lines) should converge towards the midline with an inclination progressively increasing from the anterior to the posterior sectors. This gives fullness and brightness to the smile.
Intra-dental (ratio between the height and width of each tooth) and inter-dental (ratio between the sizes of the various teeth) proportions should respect the balance of the golden ratio (Fig.3).
Particularly, in a young smile and especially in females, the “dominance of central incisor” should be present; in other words, the maxillary central incisors should be slightly larger and longer than lateral incisors to give lightness to the smile.

The incisal margins of upper teeth should follow the lower lip line while smiling; thus, proceeding from the front to the rear sectors, the curvature made up of all the incisal margins and occlusal cusps should progressively move upwards (Fig. 4, yellow line).
The gingival parabolas should be rounded and well balanced, following the cervical margins of the teeth. The gingival margins of the maxillary lateral incisors should be about 1 mm more coronal (Fig. 4, blue arrows) than those of central incisors and canines (Fig. 4, black line).

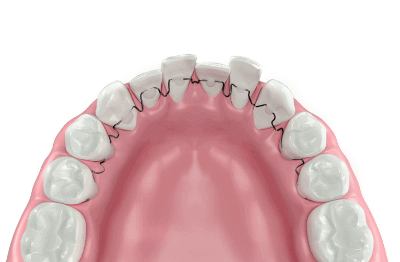
The interdental papillas should never present black triangles between teeth (indicating loss of periodontal tissues) but they should fill the entire space between the interdental surfaces of the various teeth, moving progressively in the apical direction (upward) from the front to the rear areas (Fig. 5, red triangles).
The interdental embrasures are the spaces between the incisal margins of teeth; such spaces should be minimal between the maxillary central incisors and open up progressively moving to posterior regions (Fig.5, dotted yellow line). An incorrect management of these spaces can give the sensation that all the teeth are joined together (as in case of unnatural and anti-aesthetic bridges).

The color and surface texture (the set of macro- and microscopic features of teeth and gums surfaces) should be properly integrated in each patient’s face. The teeth tend to become more and more yellow or grey (transparent) with age, due to aging and wear phenomena; the color can be corrected by dental whitening or with prosthetic reconstructions (crowns and veneers). The gums should have a coral pink color; alterations of the color, especially towards red or purple, are indicative of periodontal problems like gingivitis and/or periodontitis in the case of natural teeth and mucositis and periimplantitis in the case of dental implants.
All these parameters need to be thoroughly analysed before any dental treatment aimed at restoring the balance of the smile. The aesthetic diagnosis is performed by clinical examination as well as shooting photographs and videos. Subsequently, the study models have to be analysed in an articulator and specific softwares allow to simulate virtually the treatment on a computer before making any treatment on the patient.
At rest, a young and well balanced smile should show 1-2 mm of the incisal margins of the maxillary central incisors (Fig. 6-7-8); if such teeth cannot be seen at rest, the smile takes on an old-fashioned and anti-aesthetic appearance, as it happens with aging when the loss of elasticity of perioral tissues and bone resorption causes an inward drop of the upper lip. Such a defect can be corrected prosthetically (with veneers or crowns) or by orthodontics.
Similarly, the back teeth and in particular the upper premolars can be tilted slightly outward, so as to fill the black spaces that are sometimes seen in both sides of the smile (named as “buccal corridors”), giving fullness and brightness to the smile.




A gingival smile (or gummy smile) is characterized by the excessive exposure of the gums while smiling; even though it does not represent a functional problem, this feature is often perceived as anti-aesthetic by patients. Even in this case, the correction can be made by orthodontics, periodontal surgery and prosthodontics, according to a multidisciplinary approach aimed at restoring an harmonious relationship between teeth and gums while smiling.
The above mentioned features represent a set of parameters that must be carefully evaluated by the dentist for each individual patient, considering that the individual characteristics of each person both at rest and during dynamic functions (smiling, phonetics, chewing) are quite different. Graphs and geometric schemes should represent only the starting point to individualize the interventions and restorations needed to restore balance and brightness of the smile of each single patient.
Mock-up
It is possible to pre-visualize three-dimensionally the final result of an esthetic treatment by means of a non-invasive technique known as “mock-up”. Synthetically, this approach allows for trying-in intraorally the final prostheses before starting the treatment.
The mock-up is based on the reproduction of the ideal shape of the teeth to be treated by means of a computer or a dental master cast and permits to fabricate a silicone template (also using 3D printers) used to transfer resin composite materials intraorally, onto the intact teeth without any prosthetic preparation, just like very thin contact lenses.

This allows the patient to evaluate the possible esthetic result and the dentist to check occlusal functions (chewing, speech, etc). The mock-up technique is not invasive (it does not necessitate enamel preparation) and completely reversible: if the patient does not like the result, the mock-up can be easily removed without modifying the original shape of the teeth and with no damage for dental tissues.
Moreover, the mock-up can be easily modified intraorally, adding or removing resin materials or modifying the shape and volume of the teeth.
 Senza mock-up
Senza mock-up
 Dopo il mock-up
Dopo il mock-up
 Mockup a riposo
Mockup a riposo

Furtehrmore, the mock-up can be useful to simulate gingivectomy interventions, in other words the reshaping of the gums in case of mislevelling and/or asymmetries: in such cases, the resin composite materials can be placed over the gingival tissues, in order to simulate the final result.
If it is considered satisfying, the mock-up can be used to lead the surgeon during the gingival incision, so as to match perfectly the final contour designed on the prosthetic project.
Also communication with patients is dramatically improved by the use of the mock-up technique: in fact, pictures and video can be taken to show in real time a comparison between the pre- and postoperative situations.
Frequently Asked Questions
-
All your dental veneers are made up of ceramics?
Apart from temporary veneers made up of composite resins, yes, even if they vary considerably in terms of ceramic types: feldspathic, lithium disilicate ceramics, etc.
-
Do you use specific technologies and materials? What are they?
We use forefront equipment (intraoperative stereomicroscope, sonic and ultrasonic hanpieces, etc.), highly reliable materials (high strength ceramics, last-generation enamel-dentin adhesive systems, long lasting esthetic resin cements) and production technologies certified by our dental laboratories.
-
Do I have to drill my teeth?
Not necessarily, it depends on the type of defect. If you need to increase the volume of the teeth or to close interdental spaces (diastemas), it is also possible to use no-prep techniques that do not need to prepare the teeth; however, to achieve an optimal result, this is not always possible. The aesthetic and functional success is dictated by the fact that a minimal room is created on the tooth surface to apply the ceramic veneer (0.3-0.5 mm) without generating excessive edges or overcontours especially at the level of the gums, causing over time gingivitis, not bleachable pigmentations and other various problems. For this reason, we recommend applying dental veneers only if there is an evident shape defect or after severe erosions, while slight discromies can be treated in many cases with professional whitening.
-
Stated that the veneers are very resistant, how can I prevent them from loss of retention?
To limit the risk of decementation (reported in literature at a rate of approximately 1-2%), it is mandatory to prepare the tooth properly leaving the greatest possible amount of enamel, to use reliable cements (specific resin cements for veneers) and to pay attention during chewing, limiting cutting or tearing too hard foods and avoiding parafunctional habits, like eating nails, biting pens, etc. In addition, if teeth have been significantly lengthened for functional and/or aesthetic reasons, patients should use a protective night guard.
-
At the beginning, the veneers are not visible but how long does the effect last? How can I keep the effect over time without going back to the dentist?
The risk that veneers can become detectable is related to two factors: fake aesthetic (big “movie” teeth, too white and uniform ceramic, total absence of asymmetry) and pigmentation of margins over time. To avoid such occurrences, the clinical case have to be carefully studied with the application of thin test veneers without preparing the teeth using a technique called “mock-up”, that allows the patient to have an idea of what the final result may be before drilling the teeth and the clinician to correct any drawbacks before proceeding to the fabrication of the final restorations. Furthermore, pigmentations can be made less evident by placing the preparation margins in areas that are not visible, so preparing the teeth “strategically”. In terms of aesthetic performance of ceramics, the color never changes over time; therefore they do not need whitening like natural teeth. Conversely, the color of natural teeth, roots and composite resin restorations can change. In order to limit the onset of pigmentations, patients should limit the intake of exogenous pigments (nicotine, food pigment such as carotene, etc). Obviously periodic check-ups by the dentist are critical to ensure the aesthetic success and the proper function of ceramic veneers.
-
What are the advantages and disadvantages of other (and which) interventions?
Undoubtedly, the main advantage is minimal invasiveness, compared to traditional restorations such as crowns that necessitate the drilling of the whole tooth while the preparation for veneers only affects its outside part for a few tenths of a millimeter. Certainly, the veneers are more invasive than dental bleaching but the latter does not act on shape defects. True disadvantages do not exist, apart from “relative” contradictions, that means conditions that can limit or eliminate completely the possibility to make the veneers , as in the case of severely destroyed teeth, too much wide space, lack of intermediate teeth, etc. Obviously, each case should be evaluated individually and with a multidisciplinary approach.
-
Could you describe the patients to whom you apply dental veneers?
Mostly, patient require veneers for aesthetic reasons, so dental malformations, dental malfunctions, closure of spaces (diastemata), discoloration and pigmentations, enamel defects (amelogenesis imperfecta, fluorosis). Others are treated with veneers as finishing of orthodontic treatment: when spaces remain after orthodontics and they do not interfere with a proper occlusion, the veneers are used without moving further the teeth. Others require veneers because of dental wear, when teeth are worn as a result of friction or parafunctions and they cannot see them anymore either when talking or smiling and making the patient look like older. A smaller category concerns patients who do not want to drill their teeth and therefore do not easily accept the idea of prosthetic crowns. Patients interested in dental veneers often ask questions also about the techniques and tools necessary for whitening.
-
What do these patients have in common with each other?
Essentially, a marked aesthetic requirement: straight regular teeth, white teeth, perfect and well balanced smile. Moreover, the idea of a conservative therapy that allows limited or no preparation of teeth is undoubtedly the reason why many of them choose this type of restoration. Statistically, the veneers are mostly required by women between 18 and 45 years old, although in the last few years the trend is changing.
-
Which are the differences with other patient of your dental office?
They are patients who have a strong aesthetic feeling, great attention to details and they often have very clear ideas about the shape and texture they want to get as final result. Furthermore, dental veneers are also required by patients who are very careful to complete aesthetic treatment. The procedure is generally faster than traditional prosthesis crowns and does not absolutely require the same time as a proper orthodontic treatment.
-
What do these patients fear or worry about?
The main fear is definitely the idea of drilling teeth: patients often require veneers because they want to keep their own teeth as much as possible. Then, there is the fear of breaking or losing them while eating but, as previously mentioned, these occurrences are absolutely negligible if patients follow little advice and avoid parafunctional habits.
Contact Us
Related posts
Invisible Bracketless Fixed Lingual Orthodontics
Periodontitis can be controlled
