
Do you want perfect teeth and a youthful smile?
Smile again with dental veneers

Dental veneers, also known as esthetic veneers, are thin prosthetic restorations applied to the outer surface of the teeth to correct imperfections such as stains, spacing, chips, or irregular tooth shape. These tooth coverings can be made of ceramic, composite resin, or lithium disilicate, and in some cases they do not require tooth preparation. In the latter case, they are referred to as no-prep veneers.
Why do patients choose our dental veneers?

Minimal tooth preparation
To apply dental veneers, we follow a conservative approach, with minimal tooth reduction (0.2 mm) to avoid a visible step between the veneer and the natural tooth.

Aesthetic-driven approach
We carefully evaluate every detail to preserve the natural balance of the face, also in coordination with any complementary facial aesthetic treatments.

Careful material selection
Veneers can be made from different materials. The final choice is always made together with the patient, carefully evaluating the pros and cons of each option.
For our patients, an aesthetic consultation is included to evaluate the ideal smile balance together with dentists specialized in aesthetic medicine. We treat only a limited number of cases each month to maintain the highest standards for ultra-thin veneers.
Feel confident and comfortable every time you smile.
What are dental veneers and what are they used for?
Dental veneers are thin shells applied to the enamel surface of the teeth, acting as a tooth covering to improve aesthetics or to restore chewing function following tooth wear or trauma, such as fractured teeth or chipped edges.
These prosthetic restorations can help address the effects of bruxism and teeth grinding. Dental veneers can also correct anomalies such as interdental black triangles and diastemas. They are effective for treating pigmentation and discoloration, including stains caused by nicotine and caffeine, yellowed composite restorations, and enamel defects. The application of dental veneers is carried out by Dr. Fabio Cozzolino, a dentist specialized in dental prosthetics, restorative materials, and digital dentistry.

When and where are dental veneers applied?
Dental veneers can be applied to both dental arches, on one or more teeth. They are mainly used to restore anterior teeth (incisors and canines), but in specific cases they may also be applied to premolars.
Veneers are a conservative treatment, less invasive than prosthetic crowns, but they are not always the ideal solution. When should dental veneers not be used? There are no absolute contraindications: in some cases, more conservative treatments such as tooth whitening may be preferred. In other situations, ultra-thin veneers represent the most suitable solution.
Dark or discolored teeth
Teeth may become dark as a result of trauma or endodontic treatments. In many cases, a sort of internal hematoma (bruise) forms inside the dentinal tubules due to blood leakage or chemical substances used during root canal treatments.
Dental veneers are not always necessary: they are considered when tooth whitening is ineffective and the resulting color is unsatisfactory.
Tooth whitening is always recommended before veneer placement: the lighter the base tooth color, the thinner the veneer can be.
Chipped or worn teeth
In the presence of minor chipping on the edges of anterior teeth, veneers may represent an overly aggressive treatment. The first-line approach is always composite restorations, which tend to wear over time and lose their gloss. Composite materials therefore require periodic refinishing and polishing.
When it is necessary to restore tooth function using a more resistant material, ceramic veneers are indicated and can generally be performed even in the presence of previous composite restorations.
Stained teeth
Dental veneers can help address uneven tooth color or various types of pigmentation, which may be caused by genetic conditions or the use of antibiotics (such as tetracyclines, even during maternal pregnancy). Dietary habits (consumption of colored foods and beverages) and smoking (cigarettes, cigars, pipes) can also stain the tooth surface. In these cases, however, the discoloration is usually superficial (extrinsic stains) and can be removed using microabrasive powders and polishing pastes.
Misaligned teeth or wide spaces
In cases of tooth misalignment or spaces between teeth (diastemas), the first-choice treatment is lingual orthodontics without brackets. This approach allows spaces to be closed and teeth to be realigned without altering the tooth structure.
However, orthodontic treatment requires a longer treatment time compared to aesthetic veneers. In many cases, orthodontic therapy represents a preparatory phase for the placement of ultra-thin dental veneers, allowing for minimal enamel removal.
In patients with triangular-shaped teeth and pronounced black triangles, veneers are used after orthodontic treatment to optimize tooth shape. Veneers can also be placed at the end of orthodontic therapy to further enhance tooth shape or aesthetics.
Pros and cons of dental veneers
The main advantage of dental veneers is their minimal invasiveness compared to traditional restorations such as crowns, which require full tooth reduction. Veneer preparation involves only the outer surface of the tooth (and, in some cases, the lateral surfaces) and removes just a few tenths of a millimeter of enamel.
Tooth whitening does not correct shape defects. There are no true disadvantages to veneers; however, certain contraindications may limit or completely prevent their use, such as severely damaged teeth, excessively wide spaces, or the absence of adjacent teeth.
Advantages
- Immediate and highly noticeable aesthetic results
- Correct misaligned, stained, or chipped teeth
- Stain-resistant (ceramic veneers)
- Fast treatment process (just a few weeks)
- Average lifespan of around 10 years
Disadvantages
- Irreversible procedure (enamel reduction is required)
- Not covered by insurance
- Possible tooth sensitivity
- May require replacement over time
- Limited options if the result is unsatisfactory
Before and after: how do teeth look with veneers?
The best way to evaluate the work of a prosthodontist who places dental veneers is to look at clinical cases with before-and-after images of the treatment. Photos of smiles enhanced with dental veneers clearly show how facial aesthetics can be transformed.






Types of dental veneers: how are they made?
Thanks to modern material technologies, it is now possible to use different types of veneers, ranging from highly translucent traditional feldspathic ceramics to the more recent high-strength lithium disilicate veneers. What are the characteristics of the different types of dental veneers?
Feldspathic ceramic veneers
Feldspathic ceramic veneers, when bonded using reliable adhesive techniques, ensure excellent biological integration, outstanding aesthetic results, and a high level of biomimicry, restoring the appearance and properties of natural teeth.
Lithium disilicate veneers
The excellent mechanical properties and high fracture resistance of lithium disilicate allow for the fabrication of definitive veneers even in biomechanically challenging situations, such as in bruxism patients or in cases of severe incisal edge wear.
Zirconia veneers
Zirconia is a highly resistant material, but it presents some limitations when used for dental veneers. It has a more opaque appearance compared to feldspathic ceramics or lithium disilicate. However, new multilayer zirconias have significantly improved translucency.
Which type of dental veneer suits your smile best?
How are thin dental veneers applied to the teeth?
Minimal preparations limited to the dental enamel are available, or even treatments that do not involve altering the tooth surface at all, using additive restorations (the no-prep technique). This makes it possible to create aesthetic dental veneers with an average thickness of about 0.5 mm, helping patients achieve a perfect smile.
The no-prep technique is often combined with partial coverage of the teeth and the creation of additive partial restorations. When it is not necessary to cover the entire surface of one or more teeth, small ceramic fragments can be fabricated and bonded to the teeth.
What to do before getting dental veneers
Before creating the final dental veneers and covering the teeth, patients undergo an aesthetic try-in using temporary veneers — the mock-up — without any tooth preparation.
The process is well defined. After taking impressions, which are necessary to study the case and develop a personalized treatment plan, the ideal tooth shape is designed. This procedure allows the fabrication of special guides used to apply a thin layer of resin directly onto the patient’s teeth, enabling a preview of the final result.
These restorations do not interfere with periodontal health, as the preparations do not extend to the gingival margins, while still ensuring optimal integration and natural appearance thanks to the use of highly aesthetic, metal-free materials.

Digital Impression for veneer placement
Veneer preparation is a minimally invasive technique, and today it is possible in most cases to use intraoral scanners (Intraoral Scanner – IOS) to obtain a digital impression, without the need for impression trays, pastes, or traditional impression materials.
Intraoral scanners are high-resolution cameras that accurately capture the morphology of the teeth and gingival tissues, as well as the color of the tissues, allowing veneers to be designed and fabricated using a fully digital workflow. The digital file obtained from the scan is sent to the dental laboratory, where the restorations are produced using a completely digital process, significantly reducing manufacturing time.
How does the no-prep veneer technique work?
The no-prep technique allows veneers to be bonded to the teeth without tooth reduction. The dental surfaces are conditioned using air-abrasion powders and adhesive systems. In line with minimally invasive dentistry principles, this approach preserves tooth structure and does not compromise dental strength.
Specific clinical conditions are required to place dental veneers without tooth preparation, such as the presence of diastemas (spaces between teeth), the need to increase tooth volume and/or length, or to improve the appearance of mildly misaligned teeth. Today, ultra-thin lithium disilicate restorations (full veneers) can be fabricated in cases where complete coverage of the tooth surface is required. The reduced thickness of these restorations (up to 0.3 mm) allows for minimally invasive tooth preparations.



Restore your face with a youthful appearance: gain 10 years with the veneers
The visibility of the maxillary incisors at rest -not when smiling, but when the lips are slightly parted and during speech – is approximately 3 mm in women and 2 mm in men at the age of 25.
As time passes, this visibility decreases by about 1 millimeter every 10 years. This is why, in older individuals, the upper teeth tend to be less visible or not visible at all. We carefully evaluate the correct balance between facial aesthetics, lip support (including cases of poorly executed filler treatments), and dental veneers. By restoring the proper visibility of the maxillary incisors, it is possible to achieve a noticeably younger appearance – often up to 10 years younger.
The patient shown in the photo requested a consultation because, even when smiling, her shortened teeth were barely visible and provided insufficient support to the upper lip, which appeared thinner and slightly drooping. Worn teeth contributed to a tired and aged smile due to the loss of youthful dental proportions. Our treatment focused on a comprehensive facial analysis to identify the most appropriate solution to restore overall harmony. Lithium disilicate veneers – capable of restoring length, volume, and brightness – allowed the patient to achieve significant facial rejuvenation through a minimally invasive approach, thanks to these ultra-thin dental restorations.
Aesthetic diagnosis before and after veneers
Aesthetic diagnosis evaluates the factors that allow dental veneers to be harmoniously integrated, influencing both the smile and the overall facial appearance. This diagnosis is based on facial analysis, used to assess facial symmetry and proportions, and dental analysis, which allows evaluation of the relationships between teeth and surrounding tissues.
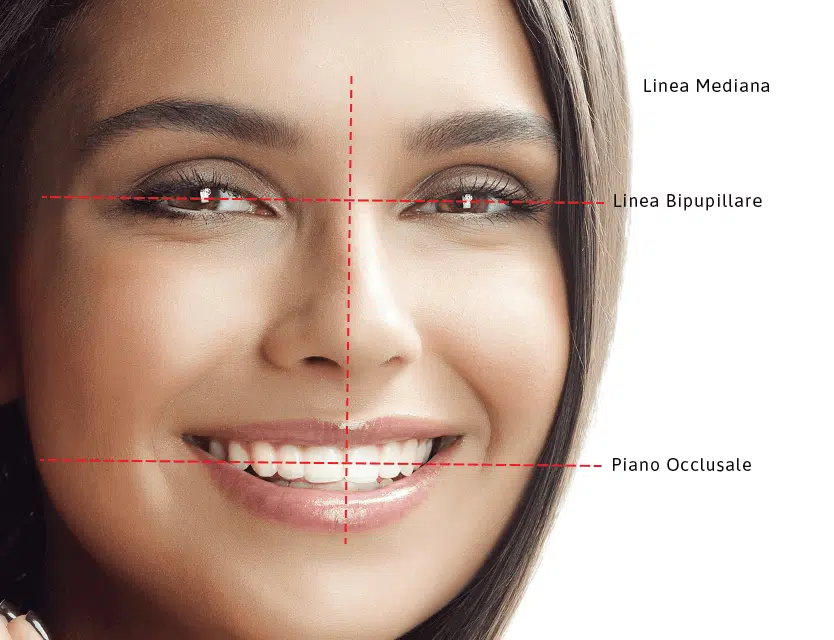
Why is facial analysis important?
Facial analysis considers the facial midline (forehead–nose–chin), the interpupillary line (passing through the pupils), and the occlusal plane (touching the incisal edges). This assessment makes it possible to identify asymmetries that need to be compensated during dental treatment, such as a canted smile line or deviations of the dental midline.
Dental analysis evaluates a series of parameters involving both teeth and gingival tissues. These include the maxillary and mandibular midlines, tooth axial inclinations, intra- and inter-dental proportions, as well as incisal curvature and margins.
Treatment planning for veneers coverage
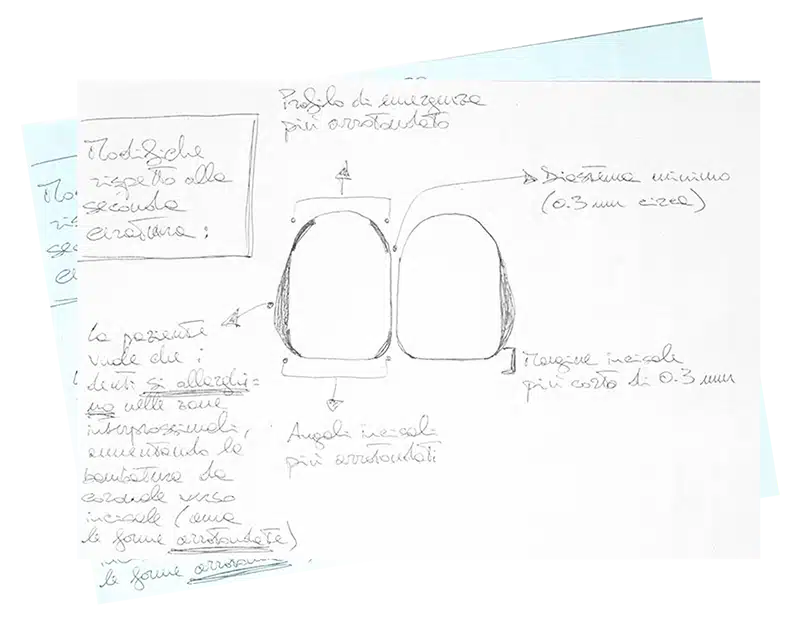
We analyze how the teeth should be covered with veneers. The maxillary midline (Fig. 1, yellow line) and the mandibular midline should coincide, and the longitudinal axes of the teeth (black lines) should converge toward the midline with increasing inclination from the anterior to the posterior sectors.
Intra- and inter-dental proportions should follow harmonious ratios based on the concept of the golden proportion (Fig. 3). The gingival parabolas should be rounded and harmonious, following the cervical profiles of the teeth. The gingival margins of the maxillary lateral incisors should be positioned approximately 1 mm more coronally (Fig. 3, blue arrows) than those of the central incisors and canines (Fig. 3, black line).


Interdental embrasures: a definition
Interdental embrasures are the spaces between the incisal edges of adjacent teeth. They should be minimal between the maxillary central incisors and progressively increase toward the posterior sectors (Fig. 4, dashed yellow lines).
Incorrect management of these spaces may create the impression that the teeth are fused together.
Additional topics for further insight into dental veneers
The average lifespan of an esthetic dental veneer is approximately 10 years, similar to any fixed prosthetic restoration. However, with proper maintenance and regular professional care, veneers can last more than 20 years.
The listed price for dental veneers varies significantly depending on the clinician’s expertise, the techniques used, and the materials selected. At Studio Dentistico Cozzolino, the cost of dental veneers ranges from €600 to €1,500 per veneer.
Temporary veneers are provisional restorations placed on the teeth to allow the patient to preview the expected outcome of the definitive veneers before final fabrication and bonding.
The choice between veneers and crowns depends on the specific clinical condition of the teeth. Crowns are indicated when a tooth is severely compromised due to caries, fractures, or large existing restorations. Whenever comparable esthetic and functional results can be achieved, the preferred approach is the least invasive treatment option for the patient.
Patients often express concerns about veneer debonding, longevity, and whether tooth preparation (reduction) is required. Another common question is what happens to the natural teeth underneath the veneers. These represent the most frequent concerns patients seek clarification about.
There are several alternatives to dental veneers. Teeth whitening represents the least invasive option when the main concern is discoloration or yellowing. Dental crowns, on the other hand, cover the entire tooth rather than only the facial surface and are indicated when the tooth is severely compromised. When the primary issue is tooth alignment, fixed or removable orthodontic appliances may be the most appropriate treatment choice.
In selected cases, veneers may provide a solution for mild misalignment, diastemas, or minor morphological discrepancies. It is important to consider all available treatment options when addressing minimal esthetic defects.
Do you want a beautiful and natural smile?
Contact us today.
Our team is available to assist international patients, provide clear information, and support you before and during your visit to Naples.
- Phone: +39 081 245 1805
- Email: info@studiodentisticocozzolino.it
- Address: Via Raffaele De Cesare 31, 80132 – Naples, Italy
We recommend contacting us in advance to better organize your visit and ensure the best possible care. Ask for info or schedule a visit.
